

Peripheral Angioplasty
 Home
Home- Peripheral Angioplasty

Medically Reviewed By Dr. Antariksh Vijan Updated on June 01, 2026
Peripheral angioplasty is a minimally invasive procedure used to open blocked or narrowed blood vessels in the legs and parts of the body outside of the heart. The condition it addresses is peripheral artery disease (PAD). Think of it like coronary artery disease, excluding heart, it commonly happens in the arteries of legs, but can also happen in neck, arms & kidneys. Arteries develop blockages, which in turn obstruct blood flow. When this does happen, a person may experience pain walking, or in some cases the condition may manifest through sores that don’t heal easily. In cases of extremely low flow, amputation can be a risk. The procedure itself resembles coronary angioplasty, in terms of mechanics — doctors pass a thin tube with a small balloon into the blocked artery and gently inflate it to restore blood flow; sometimes a tiny metal scaffold (stent) is also placed to keep it open. It can dramatically reduce pain and even restore walking ability. Sores, if present, may heal. In more extreme cases, it can be the difference between saving and losing a limb.
Today, well over 200 million people live with peripheral artery disease, with some studies estimating that 1 in 20 Indians may be affected. Some studies suggest that 1 in 4 high risk individuals may be affected in India. Peripheral artery disease prevalence in India is driven by diabetes, smoking, hypertension and dyslipidemia.
Conditions Treated with Peripheral Angioplasty
“It’s just…leg pain, from age”. That’s not uncommon to hear — persistent leg pain is a reasonable indicator for peripheral artery disease, which is the main condition addressed by peripheral angioplasty. In simple terms, peripheral artery disease (PAD) means arteries outside the heart — mainly in the legs — have become narrowed or blocked by fatty deposits.
When this happens, blood can’t flow properly to muscles and skin. They might experience pain or cramping in the thighs or calf when walking that eases with rest (claudication). They can also experience cold feet, dark or pale toes, or slow healing cuts and ulcers. In more severe cases, there may even be pain at rest.
PAD is caused by atherosclerosis. While most common in the legs, it can also affect the pelvic area and sometimes renal/subclavian arteries.
Key Indications by Territory
In the lower limbs, intermittent claudication is the classic indicator — pain that eases with rest. When the condition worsens, the pain persists even at rest. Ulcers may show up; these can take very long to heal or simply persist. In very severe cases, the blood flow is reduced to such a point that gangrene may develop. This classifies as ‘critical limb ischemia’, and could be grounds for amputation. While significantly less common, stenosis can also occur in the renal artery. Typical indicators are hypertension that’s resistant to medication and kidney function that’s progressively worsening. In some cases, the iliac, femoral, popliteal or tibial arteries could be affected. This manifests through pain while walking, and in more extreme cases, limb loss may be a risk.
In India, unfortunately, many patients present with critical limb ischemia rather than early claudication. Many Indian studies also point towards a high-burden of multilevel and below-knee disease in diabetics.
Indications for peripheral angioplasty:
Peripheral angioplasty is not for every blockage; doctors look for certain scenarios in which angioplasty is likely to really help and would justify the potential risks involved.
It is usually advised when leg symptoms are strong enough to limit everyday life, despite medicines, walking exercises and therapy, and risk factor management. For example; if someone has to stop every few minutes because of pain and can no longer do simple daily tasks, angioplasty may merit consideration. Angioplasty is considered if the limb is at serious risk — this means constant pain, even at night/at rest, dark or blackish-blue toes, or any early signs of gangrene. In these situations, if blood flow is not restored with urgency, irreversible damage may occur which in turn might lead to amputation being the only course of action. As with coronary artery disease, angioplasty and surgery are treatment options. Here, doctors will consider overall health and comorbidities — in particular kidney function — and the placement of the blockages while deciding on a line of approach.
Contra‑indications include severe contrast-dye allergy, advanced kidney failure, uncontrolled infection or very diffuse disease where surgery may be better.
Reference - Angioplasty and stenting for peripheral arterial disease of the lower limbs: an overview of Cochrane Reviews (Protocol). Cochrane Database of Systematic Reviews, CD012542. [PMCID: PMC6464525]
Peripheral Angioplasty Procedure: Step-by-Step Flow
- Pre-procedure workup: Like any procedure, this involves clinical examinations and monitoring of vitals. There’s a routine of tests including ABI, Doppler/CTA/MRA, blood work, renal function, ECG and optimization of BP and diabetes meds. Anti-platelets may be started or optimized. There is ideally a detailed discussion about the risks and need to switch over to surgery, in case of critical limb ischaemia.
- Access and diagnostic angiogram: Not unlike a heart patient, where an angiogram is required to map out the blockages. If feasible, interventional radiologist performs angioplasty via the same catheter setup. The procedure is usually done in a cath lab, under local anesthesia. The common approach is the femoral artery, however, radial or pedal access is increasingly used for patients where it may be the favourable approach. A sheath is placed and a contrast angiogram maps the lesions. Following this, the actual angioplasty can happen.
- Crossing the lesion: A guidewire is navigated through the stenosis or occlusion (intraluminal or subintimal track) under fluoroscopy (live X Ray). In long or more tortuous (curvy) segments, a diagnostic catheter may be used to support the wire passage.
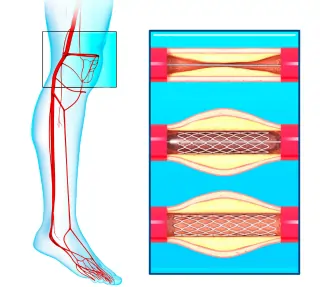
- Balloon Angioplasty (PTA): This is the core of the actual procedure. A balloon catheter, which is appropriately sized for the vessel diameter, is placed over the guidewire, across the lesion. The balloon is then gradually inflated (several seconds to minutes, depending on the state of the vessel) to crack or compress the plaque and ‘open up’ the vessel.
- Stenting/adjuncts as required: In case of persistent stenosis, flow-limiting dissection or elastic recoil, a bare-metal or drug-eluting stent (usually nitinol for SFA) is placed. For calcified/difficult lesions, atherectomy, scoring/cutting balloon, or a drug-coated balloon can be done. With calcification, the arteries get stiff and hence, expanding them becomes more challenging. It needs to be with enough care to not cause a crack or any damage to the vessel.
- Completion and haemostasis: A final angiogram evaluates luminal gain, distal runoff, and collaterals. The sheath is then removed. Manual compression or a vascular closure device is used to seal the hole, after the sheath comes out. The patient is monitored for a few hours. Discharge is usually on the next‑day or sometimes, the same‑day, depending on complexity
Advances in Peripheral Angioplasty Technology
- Drug‑coated balloons (DCB): Balloons coated with antiproliferative drugs (e.g., paclitaxel) reduce restenosis and reintervention in femoropopliteal disease in many trials.
- Modern nitinol stents and stent-grafts: Flexibility and resistance to crushing in case of movement in the SFA and popliteal arteries; covered stents for treatment of long lesions or aneurysms.
- Atherectomy devices (rotational, orbital, laser, directional): These are useful for the removal of calcified plaque to improve luminal gain and allow better balloon expansion, especially in below‑knee vessels.
- Chronic total occlusion (CTO) crossing/entry devices: Aid in traversing long CTOs in SFA or iliac arteries that earlier went straight to bypass surgery.
- Radial/pedal access and hybrid operating rooms: Help in conducting multiple levels of interventions with increased patient comfort and reduced bleeding risks.
Reference: Recent advances in endovascular treatment of peripheral arterial disease. F1000Research, 9, 122. [PMCID: PMC7043107]
Benefits of Peripheral Angioplasty
When done for the right patient, peripheral angioplasty can offer several meaningful benefits.
Relief from leg pain and cramps:
By improving blood flow, it takes care of rather debilitating pains and significantly improves the quality of life. Many people can walk further with little to no calf or thigh pain. Social life can restart, daily tasks like grocery shopping become possible. For those living or working on higher floors, climbing stairs becomes possible again. Just taking a casual evening stroll becomes easier again.
Better healing of wounds and ulcers:
If blood supply improves, slow‑healing cuts, diabetic foot wounds, or small areas of gangrene are more likely to heal, especially when there is proper management of diabetes and infections. There is a reduced risk of amputation in cases where wounds fail to heal.
Limbs salvage in advanced cases:
In advanced PAD which presents with pain at rest, blackened/bluish toes, or ulcers, restoring circulation quickly may be the difference between keeping and losing the limb. A timely angioplasty could be crucial.
Minimally invasive with quicker recovery:
The procedure is done via a tiny hole made at the groin, arm, or foot, and is usually performed under local anesthesia. Compared to open surgery, hospital stay and recovery are generally quicker especially for older and more frail patients.
Risks and Complications
Every procedure comes with its own risks and complications. Luckily, with peripheral angioplasty, the risks are relatively low but not non-existent. Here’s a basic breakdown:
Problems at the puncture site: Because angioplasty is done through a small artery in the groin, arm, or foot, there can be bleeding, bruising, or a lump (haematoma). Very rarely, a small ballooning (pseudoaneurysm) or connection between an artery and vein can form and may need treatment.
Issues inside the artery: During the process of opening the blockage, the artery can tear (dissection), especially if it’s very calcified and stiff, or small bits of plaque can travel downstream and block smaller vessels. This could reduce blood flow and require urgent repeat angioplasty or surgery.
General medical hazards: There is a small chance of heart attack, stroke, allergic response to the dye or kidney strain. Especially in older patients who are diabetic, have kidney or heart issues. In the long term, the treated artery can narrow again (restenosis) and this could require another procedure. Some studies report medical morbidity in 2-3% of the cases, after the procedure.
Recovery and Rehab
Recovery from peripheral angioplasty is usually pretty seamless, but the process still needs care and discipline.
First 24–48 hours:
The patient will usually lie flat for a few hours so the puncture site in the groin, arm, or foot can seal. Soreness or bruising is normal; however, severe pain, swelling, or fresh bleeding should be reported immediately. Most people go home the same day or the next day, with advice on how much to walk and how to care for the dressing.
Weeks 1-2:
Light walking is encouraged — short, frequent walks on level ground, gradually increasing distance. Heavy lifting, squatting, or running is to be avoided until doctors give clearance — this tends to vary from case to case. It’s very important to monitor feet, on a daily basis, for colour changes, temperature drop or new wounds, especially if the patient is diabetic. Blood thinners are usually prescribed.
Long-term rehab:
This phase involves supervised or structured walking programmes, with a close eye on blood sugar levels and blood pressure levels — these are the usual culprits affecting long term recovery. Strict sugar and blood‑pressure control. Obviously, healthy eating is everything — less fried food, sugary food, red meat and salt. Given the still alarming number of smokers in India (over 100 million people), it’s worth mentioning that smoking contributes to atherosclerosis. It’s mandatory to reduce smoking to keep the artery open and avoid any restenosis.