

MICS CABG Surgery | Minimally Invasive Heart Bypass Grafting
 Home
Home- MICS CABG Surgery | Minimally Invasive Heart Bypass Grafting

Medically Reviewed By Dr. Vishal Pingle, Cardiothoracic & Heart Transplant Surgeon. Updated on Feb 9, 2026
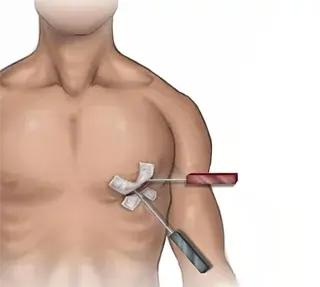
MICS CABG Surgery is a modern alternative to the traditional bypass. Instead of opening the entire chest through a sternotomy, surgeons make a small incision between the ribs (6-10 cm) on the left side of the chest. The breastbone is not divided, which makes the process less invasive.
Brief About CABG Surgery
A Coronary artery bypass graft, commonly referred to as CABG, is a surgical procedure performed for patients who’ve been diagnosed with Coronary artery disease (CAD) or Ischemic heart disease (IHD).
Coronary Artery Disease is a cardiovascular disease characterized by the narrowing of coronary arteries (vessels that supply the heart muscles with blood), due to the build up of cholesterol and other substances, collectively known as atheromatous plaque. A CABG is conducted by taking a healthy blood vessel from another part of the body — typically the legs, arms, chest or wrist — to make a new pathway for the flow of blood and oxygen to the heart — essentially, bypassing the old blocked pathway. The new pathway is called a graft.
The CABG procedure has been around for almost 60 years now. Dr. Rene Favaloro is credited with performing the first successful modern-era CABG, in 1967. His procedure of using the saphenous vein graft became the standard for the next two decades. By the 1980s, total arterial revascularization became possible. By the 1990s, patient outcomes improved due to advancements that allowed a ‘beating heart’ surgery (a CABG performed without the assistance of a heart-lung machine) and post the 2000s, minimally invasive techniques were used along with robotic assistance too.
These advancements can help us understand the differences between procedure and approach. Essentially, procedure indicates the type of surgery that is being conducted (for example; CABG Surgery or Valve Replacement). Approach indicates HOW the surgery will be conducted (open-heart, minimally invasive, robotic assistance, etc).
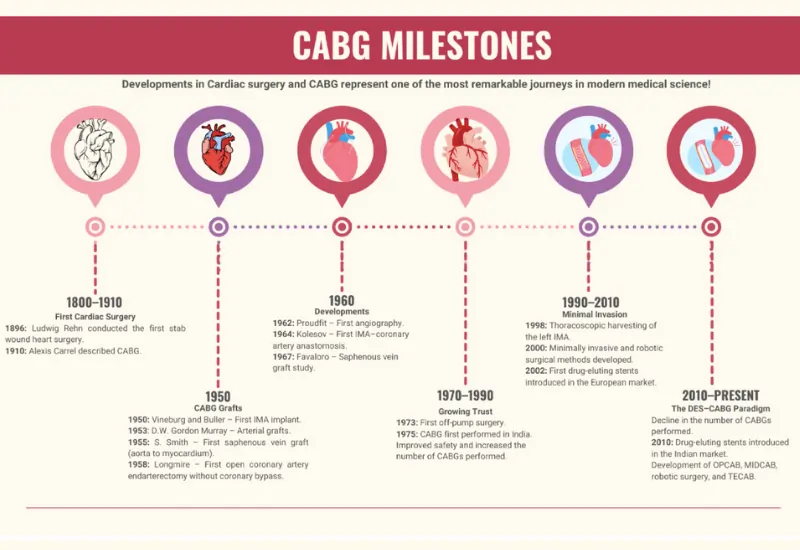
Image credit: Unsung Heroes of Coronary Interventions (Journal of Vascular Diseases).
Open Heart CABG & MICS CABG Surgery
If your surgeon has suggested bypass surgery as an intervention, there are typically two possible approaches:
A traditional open-heart surgery: This is also known as a median sternotomy. A surgeon will make an incision down the middle of the chest and carefully divide the breastbone (sternum) to reach the heart. This wide opening allows the surgical team to clearly access the heart and surrounding blood vessels, and perform the operating procedures with precision.
After the surgery, the breastbone is closed with surgical wires to ensure it heals properly, and the skin is stitched or stapled shut. Patients usually spend a few days in the intensive care unit, followed by a hospital stay of about a week. Full recovery can take several weeks, as the breastbone needs time to heal completely.
Minimally invasive coronary artery bypass grafting (MICS CABG Surgery): The surgeon performs surgery through small opening using specialized instruments. As in a standard bypass, a healthy blood vessel from another part of the body–usually the legs or chest–is used to reroute blood flow around blocked coronary arteries restoring oxygen-rich blood supply to the heart.
Because the chest bone remains intact, patients often experience lesser pain, shorter hospital stays, quicker return to daily activities, and fewer complications compared to traditional open-heart surgery. However, not every patient is eligible for this procedure–eligibility depends on various factors including number of blocked arteries, overall health and other medical conditions.
Diagnosis & Eligibility for MICS CABG Surgery
aBefore recommending a bypass surgery, doctors usually carry out a series of diagnostics tests to understand how well your heart and blood vessels are working. The goal is to see where your blockages are, how severe they are, and what form of intervention is suitable for you.
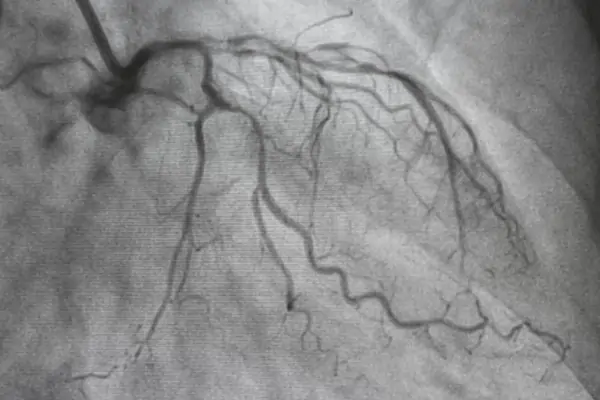
The most important test is a Coronary Angiogram (CAG). In this procedure, a thin tube (catheter) is gently guided through an artery–usually the radial artery in the arm, or the femoral artery, near the groin–to your heart. A special dye is then injected, which makes the coronary arteries visible on X-Ray images. This shows where and how much narrowing has occurred.
Doctors may also use echocardiography (ultrasound of the heart) to check heart function, and blood tests, stress tests and other forms of testing to measure overall heart health.
Upon reviewing these tests, your cardiologist and surgeon will decide:
- Whether you need a bypass
- How many grafts are required
- If you are suitable for MICS CABG or a traditional bypass.
Specific eligibility criteria for MICS-CABG:
You may not be considered a good candidate for MICS-CABG if:
- You have multiple blockages in different arteries (multi vessel disease), that require several bypass grafts
- Your heart function is weak or your heart muscles have been damaged by previous heart attacks
- You have severe lung disease or extreme obesity, which limits access to the heart through a small incision
- There are blockages in your heart that cannot be reached safely without opening the breastbone
You may be considered a good candidate for MICS-CABG if:
- Your blockages are located in arteries that can be easily accessed through the small incision between the ribs (most often the left anterior descending artery)
- Your heart function is stable; you do not severe enlargement of the heart (cardiomegaly) or very weak heart function
- You need one or two bypass grafts, rather than several grafts across different areas of the heart
- You do not have other medical conditions that make the procedure complicated — like chest deformities, obesity or advanced lung disease
- You’ve had a previous heart surgery and/or, this is a repeat bypass
Difference Between Open Heart CABG & MICS CABG Surgery
| Feature | Sternotomy (Open CABG Surgery) | MICS CABG Surgery (Minimally Invasive CABG) |
|---|---|---|
| Incision | Long incision down the middle of the chest (8–10 inches), breastbone divided | Small incision (6–10 cm) between the ribs, breastbone intact |
| Access to Heart | Full view of the heart and all coronary arteries | Limited access; suitable for selected arteries and patients |
| Use of Heart–Lung Machine | Commonly used (on-pump CABG) | Often performed on a beating heart (off-pump), though machine may be added if needed |
| Pain & Recovery | More pain due to breastbone healing; 8–12 weeks recovery | Less pain; faster recovery (4–6 weeks) |
| Hospital Stay | 7–10 days | 4–6 days |
| Scarring | Large mid-chest scar | Smaller scar on the side of chest |
| Suitability | Suitable for all types of coronary disease, including complex multi-vessel and left main disease | Best for 1–2 vessel disease, selected multi-vessel cases, not always suitable for complex cases |
| Complications | Higher risk of wound infection, sternal non-healing in diabetics/obese patients |
Lower risk of infection, fewer wound complications
|
As published in a PubMed Central (PMC) – Review on new advances in minimally invasive coronary surgery shows that both short-term and long-term outcomes of MICS CABG are favorable, with reduced postoperative morbidity and comparable long-term survival to conventional coronary bypass surgery.
Step-by-step guide to preparing for MICS CABG Surgery
If your doctors have recommended an MICS CABG Surgery, here’s is what typically happens:
One to two weeks before the surgery:
- Your doctor will review your test results and confirm you are fit for surgery
- If you are on blood-thinning medications (like Aspirin, Clopidogrel or Warfarin), you may be advised to stop or reduce them several days before, to reduce bleeding risk
- You may be asked to start gentle breathing exercises to strengthen your lungs
One to two days before the surgery:
- You will be admitted to the hospital, usually a couple of days before the procedure
- Doctors and nurses will check your vital signs, review tests and answer any questions you may have
- Blood tests, chest X rays, or other final scans may be repeated
The night before:
- You will be asked to fast (no food or drink) for about 6-8 hours before the surgery
- Any areas where grafts will be taken (leg, chest or arm) may be cleaned and prepared
After surgery:
- Expect 1-2 days in the ICU monitoring, followed by 3-4 days of hospital stay
- Most patients are able to walk within 1–2 days, are discharged within 3–5 days, and can return to normal activities in 2–3 weeks
What Makes a Surgery Successful?
Upon returning to normal activities, you’d notice a significant improvement in day-to-day symptoms. Here are some to watch for:
- Reduced chest pain or heaviness (angina): Activities that once caused a lot of difficulty — like climbing stairs, carrying loads, or even walking — can now be done with much more ease. You will notice a significant relief in your chest area
- Improved endurance and stamina: You will find it significantly easier to walk longer distances, without the need for a break. Additionally, you will find that daily tasks like bathing, cooking and dressing no longer feel tiring
- Better quality of sleep and rest: Night time chest discomfort and breathlessness is much less common
Doctors may confirm success through follow up tests (like ECG, Echocardiogram, or stress tests), but for a patient, the clearest sign is being able to return to daily life with less pain and greater ease.
Risks & Possible Complications of MICS CABG Surgery
Like any surgical procedure, MICS CABG Surgery carries some risks. Although the minimally invasive approach often means less pain, faster recovery and fewer complications compared to traditional open-heart surgery, it’s still important to be aware of some potential outcomes.
Common risks include:
- Bleeding during or after the operation
- Infection at the incision site, though this is less likely than with a sternotomy
- Irregular heart rhythms (arrhythmias), which are usually temporary
- Reactions to anaesthesia or other medications
Less common, but more serious risks include:
- Stroke or heart attack during or after the surgery
- Graft failure, where the new vessel does not stay open
- Lung or breathing problems, especially in patients with pre-existing lung disease
Surgeons often use risk-calculating tools to estimate the risk of mortality. However, it’s important to note that outcomes can vary. Largely, it depends on how sick the patient is prior to the procedure, the complexity of the operation, and the expertise of the surgical team.
What happens if complications arise?
Although MICS-CABG is designed to be safe and less invasive, there are situations where the surgical team may need to change the approach during the operation.
- Conversion to sternotomy: In rare cases, if bleeding cannot be controlled or the arteries cannot be reached safely, or the anatomy is more complex than expected, the procedure may be switched to a full sternotomy (opening the breastbone). This gives the surgeon complete access and ensures the operation is done safely.
- Use of a heart-lung machine: Most MICS-CABG surgeries are performed with a beating heart, without this machine. However, if the heart becomes unstable or the blood pressure drops, the team may connect you to a heart-lung machine for added safety.
These scenarios are planned well in advance, to protect a patient if unexpected challenges arise.
Repeat bypasses and choice of grafts:
Sometimes, patients who’ve had bypass surgery in the past may require a repeat bypass if the grafts placed earlier become blocked over time. MICS-CABG is used for repeat procedures as well, with good long-term outcomes.
In any bypass surgery, however, the choice of graft material is important. Surgeons can use either arterial grafts (blood vessels from the chest or arm) or venous grafts (usually from the leg).
- Arterial grafts tend to stay open longer and provide better long-term results, especially for crucial arteries like the left anterior descending (LAD) artery.
- Venous grafts are more commonly available and can be used to bypass multiple blockages, but they tend to narrow or close earlier than arterial grafts.
In some patients, surgeons aim for total arterial revascularization, using only arteries to maximize durability and long-term heart health.
Questions to Ask Your Doctor
If you’re considering MICS CABG Surgery or have already been advised to undergo bypass surgery, it’s important to have a clear understanding of your options. Here are some useful questions to ask your doctor:
1. Is MICS CABG the better option or traditional sternotomy? Why?
2. How many grafts will I need, and which arteries will be treated?
3. In my specific case, what are the risks and how do they compare to the average risk?
4. How do you measure the risk levels?
5. What is the chance that my procedure may be converted to a sternotomy or require a heart-lung machine?
6. Why was I recommended for bypass surgery and not coronary angioplasty?
7. If I choose not to have surgery, what are my options? And, what are the possible outcomes?
8. Have you treated patients with a similar case profile? What were the outcomes?
9. Will you be using arterial grafts or venous grafts? Is a total arterial revascularization possible, in my case?
10. Can I reschedule my surgery? If so, what’s a safe timeline?
11. What is the expected recovery time, in my case? When can I return to work, exercise or daily activities?
12. What should I AVOID after the surgery?
13. Will I require cardiac rehabilitation after surgery, and what does it involve?
14. What long-term changes will protect the success of my bypass?
15. Is there an age-limit for bypass surgery?
Asking these questions will help you make a more informed decision, and feel more confident about your treatment plan.
Infrastructure Required For MICS CABG Surgery
Not every hospital has the necessary infrastructure for a bypass surgery.
Bypass surgery infrastructure includes advanced diagnostic imaging, specialized cardiac surgery suites, state-of-the-art monitoring and surgical equipments, advanced heart-lung machines (for traditional on-pump surgeries), 3D CT scans and intraoperative echocardiography, robotic systems for minimally invasive approaches and post-surgical care facilities with a cardiac intensive care unit (CT ICU) with mechanical ventilation and rehabilitation programs.
We can broadly categorize hospitals into the categories of nursing homes, general surgical hospitals, multi-speciality and super-speciality hospitals.
Typically, a nursing home would have provisions for an Echo and ECG. They can alert you to a potential cardiac event. General surgical hospitals may or may not be equipped for minimally invasive procedures. Multispeciality hospitals may offer a CABG, but this largely depends on the expertise of the surgeon involved. Super-speciality hospitals tend to have everything necessary for a complex cardiac surgery, and entire centers focused on cardiac, neuro and oncological care.
| Hospital Type | Facilities | ICU Strength | Advanced Imaging (CT, MRI, Cath Lab) | Cardiac Surgery Capability | Suitability for MICS-CABG |
|---|---|---|---|---|---|
| Nursing Homes | Basic wards, limited beds | Basic or none | Usually not available | Only minor surgeries | ❌ Not suitable |
| General Surgical Hospitals | Multiple surgical departments, moderate setup | Standard ICU, limited monitoring | May have X-ray/ultrasou nd, rarely cath lab | General & routine surgeries, rare cardiac care | ❌ Rarely suitable |
| Multispecialty Hospitals | Large setup, many specialties | Full ICU with ventilators & monitoring | CT, MRI, cath lab often available | CABG possible, depends on surgeon expertise | ⚠️ Sometimes suitable |
| Super-Specialty Hospitals | Focused on cardiac/neuro/ oncology | Dedicated CCU & advanced ICU care | Advanced cath labs, hybrid OT, ECMO | Complex CABG, redo, robotic, minimally invasive | ✅ Best suited |
Seeking a second opinion and knowing your rights:
It is natural to feel anxious or uncertain, when considering cardiac surgery. You always have the right to seek a second opinion from another heart specialist–in fact, this is highly recommended. A second opinion can confirm the diagnosis, offer an alternative approach or simply provide peace of mind before making a decision.
In India, the Charter of Patient Rights (issued by the National Human Rights Commission and Ministry of Health) guarantees you the right to information, the right to informed consent and the right to choose or refuse treatment. You have the right to seek a second opinion, without discrimination or any pressure to take further services.
Rehabilitation & Post MICS CABG Surgery Care
Recovery after a bypass surgery happens in phases, rehabilitation plays a key role in healing and protecting your heart.
Immediate (first week):
You will stay in the ICU for 1-2 days, and a couple more days in the hospital. Nurses and physiotherapists will help you sit up, breathe deeply and take short walks to regain strength.
Mid-term (2-6 weeks):
At home, recovery continues with gradual return to light activities. Wounds are checked, stitches removed and pain reduces steadily. During this phase, many patients begin cardiac rehabilitation — supervised sessions with light walking, slow cycling on a stationary bike, stretching and relaxation exercises to improve stamina and confidence.
Long term (after 6 weeks):
Most patients are able to get back to their normal routines. Those who stick with a full cardiac rehab program do much better — research shows consistent rehab can reduce the risk of mortality by nearly 50%, compared to partial participation. Rehab would include a heart-friendly diet, regular aerobic exercises like brisk walking or swimming, stress management and quitting smoking if needed. With time, most patients regain strength and a better quality of life.
We usually advise patients to undergo 36 sessions (12 weeks) of focused cardiac rehab. In some cases, we may advise as many as 72 sessions.
Choosing the Right Hospital & Cardiac Surgeon
Selecting the right surgeon is the most important part of your bypass journey. Make sure you take the time to arrive at a decision you and your family are comfortable with.
Try to look for a surgeon who has specific experience with the type of procedure recommended for you. Ask how many similar surgeries they perform each year, and their success rate. The expertise of the surgeon plays a huge role in selecting an approach — some may prefer a sternotomy for complex multi-vessel disease, however another may be comfortable with a minimally invasive approach. .
Converse openly with potential surgeons, to understand their approaches. A good surgeon will take the time to explain your options, discuss risks honestly and answer your questions clearly.
- Ask or look for patient testimonials. Speaking to patients who’ve undergone MICS-CABG can provide helpful insights into a surgeon’s approach and bedside manner.
- Search recent publications and conferences for a surgeon’s work. Those who are active here tend to be at the forefront of innovation and techniques.
- Look for specialist credentials–surgeons who have advanced fellowships or training in MICS are often well-equipped for challenging cases. Some fellowships you can ask about are: MICS-CABG fellowship (EACTS), IACTS fellowship, Minimally invasive cardiac surgery fellowship from the Baylor College of Medicine, and the MICS-Heart fellowship.
- Research hospital quality metrics–such as surgical mortality rates, readmission data or patient outcomes.
- Look for a super-speciality hospital that conducts a high-volume of MICS-CABG surgeries.
Comfort, trust and open communication are as important as technical expertise.
Cost of MICS CABG Surgery in India
Understandably, this is a pragmatic factor in decision making.
The cost of an MICS CABG depends on various factors including the type of hospital (government or private), experience of the operating surgeon, complexity of the procedure and patient’s overall health. Typically, private hospitals in larger cities have higher prices.
In a government hospital, the cost ranges from ₹ 100,000 to ₹ 250,000. These costs are significantly lower than private hospitals, due to subsidized rates and lower overall overheads. However, the biggest drawback is the waiting period. Due to higher caseloads, you may face an extended waiting period for your surgery.
In private hospitals, the cost for CABG ranges from ₹ 2,40,000 to ₹ 400,000. MICS-CABG can cost between ₹400,000 and ₹ 900,000 and robot-assisted CABG can cost between ₹ 500,000 to ₹ 10,00,000
| Hospital Type | Typical Cost Range | Notes / Considerations |
|---|---|---|
| Government / Public Hospitals | Very low to modest, sometimes subsidized or free for eligible patients. ₹ 100,000 to ₹ 250,000 | In government hospitals the cost may be heavily subsidized, with patients paying only for consumables or minimal hospital fees. However, fully public MICS CABG programs are rare in many states |
| Private Hospitals | ₹ 400,000 to ₹9,00,000+ for minimally invasive / hybrid surgeries | Private hospitals charge for advanced infrastructure, surgeon expertise, consumables, ICU stay, etc. The cost varies significantly by city, hospital prestige, number of grafts, and complexity. |
The final costs of your hospital stay will also depend on factors like duration of stay, other treatments required in conjunction and the room category selected.
Once you’re discharged, there are still ongoing costs. This is considered the ‘life-cycle cost’ of a bypass surgery.
Lifelong medication will be prescribed by your doctors.
Usually these are: Beta-Blockers: To manage heart-rate and blood pressure.
Statins: To control cholesterol
Antiplatelet medications: To prevent blood clots
Other cardiac medications specific to your condition may be prescribed. Cardiac rehabilitation programs will also incur an additional cost.
Additionally, follow up consultations with a cardiologist and other specialists are crucial for monitoring and adjusting medications.
Long-term financial considerations:
‘Lifestyle modifications’ aren’t a direct cost, but they definitely influence future medical expenses. Changes in diet, purchase of exercise equipment or a gym membership, and reducing smoking/alcohol consumption all have a huge impact on your post-surgery health.