

Uterine Artery Embolization
 Home
Home- Uterine Artery Embolization

Medically Reviewed By Dr. Antariksh Vijan Updated on June 01, 2026
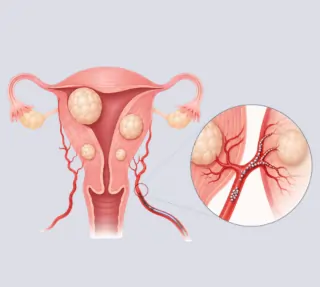
Uterine artery embolization is a minimally invasive procedure that shrinks fibroids by gently cutting off their blood supply. Fibroids are essentially non-cancerous growths made of smooth muscle cells and fibrous connective tissue.
The procedure offers relief from pain and heavy menstrual bleeding. It is performed by an interventional radiologist via a small puncture in the groin or wrist. A thin tube (catheter) is guided into the arteries supplying the uterus and tiny particles are placed to stop blood flow to the fibroids. The days following the procedure are referred to as the post-embolization period. During this time, patients can suffer mild cramping and fever. However, they recover faster than with a major surgery.
They’re often sent home the same day or after an overnight stay. Also called as Uterine Fibroid Embolization (UFE), is a strategic choice for patients choosing to preserve their uterus. Patients who would like to preserve their uterus often prefer this to a surgical intervention. The procedure reduces heavy menstrual bleeding and dramatically improves the quality of life for many women. Risks are typically uncommon, but infection is a concern. While there is no cumulative national registry, it is estimated — from various single center reports — that up to 10,000 women in India undergo the procedure each year, with success outcomes matching global data (<4% major complications).
Conditions Treated with Uterine Artery Embolization
Uterine fibroids can cause a range of symptoms depending on their number, size, and location. It’s not always a ‘critical’ situation, but can eventually take its toll on life quality.
Heavy or prolonged menstrual bleeding (menorrhagia): Many women with fibroids lose more blood than usual, have periods that last longer than seven days, or need frequent pad/tampon changes. Past a certain level, this can bring life to a halt — work, study, sport and training, even socializing. All planning revolves around it, and exhaustion is a gateway to mental health concerns too. Weakness, dizziness and chronic fatigue due to iron-deficiency anemia are some of the effects.
Pelvic pain, pressure, or a feeling of fullness: Many women have continuous aching, sharp cramping, or a feeling of “fullness” low in the belly from fibroids growing within or outside of the uterus; large fibroids may make clothes feel tight or cause visible abdominal swelling. While not ‘medical’, this creates a persistent diffidence and deeply limits choice of clothing.
Urinary bladder symptoms: Fibroids press against the urinary bladder, causing a very urgent need to urinate, or a very frequent need. Constant waking at night to urinate is common, and in some rare cases, emptying the bladder completely becomes hard. Planning social visits or travel becomes extremely hard with such a situation.
Bowel symptoms and bloating: When fibroids press toward the back, it may cause a feeling of constipation, bloating, or a need to excessively strain to pass stools.
Pain during sex and back/leg pain: Some fibroids cause discomfort during sex (dyspareunia) or radiating lower‑back or leg pain when they press on nearby nerves, not entirely unlike sciatica. A healthy sex life is essential to well being, and naturally a limitation of this nature can be incredibly debilitating emotionally and mentally, let alone physically.
Abnormal bleeding is a common presenting complaint in Indian clinics, and some regional series report that roughly two‑thirds of women with symptomatic fibroids seek care for bleeding; access to specialized treatment varies by location, so early discussions with gynecologists helps determine testing (ultrasound/MRI), blood panels can detect anemia and a further course of action is determined post these.
Indications for Uterine Fibroid Embolization
UFE is offered when fibroids are causing significant clinical symptoms and a less‑invasive option than surgery is desired — quite often, this becomes the line of thought with patients who want to preserve their fertility. These are some of the typical markers. In this case, they may resemble the conditions outlined in the previous section, but have it’s important to understand that from a symptom and treatment standpoint:
- Excessive and prolonged menstrual bleeding, which cannot be managed by medications, especially when it’s reached the stage of causing anemia and disrupting daily life.
- Bulk symptoms from an enlarged uterus or large fibroids — a sense of pressure, visible abdominal swelling, or difficulty with clothing and exercise.
- Pelvic pain or frequent cramps directly linked to fibroids, including pain that limits activity or sleep.
- Frequent need to urinate or inability to empty bladder due to the fibroid pressing on the bladder.
- Difficulty with constipation, bloating, or straining associated with bowel movements, as a result of the pressure of the fibroid on the rectum.
- Recurrent symptoms after a prior surgery, or a higher-risk profile for another surgery due to other comorbidities — in these cases, UFE is preferred over any surgical intervention.
- Desire to preserve the uterus: UFE is an alternative to hysterectomy for women who want uterine conservation and symptomatic relief.
Ultimately, UFE is an interdisciplinary discussion. While an interventional radiologist performs the actual procedure, a gynecologist helps the patient weigh against medical treatment, myomectomy (surgical removal, while preserving the uterus), or hysterectomy (total uterus removal) based on symptoms, fibroid type/location, age, and reproductive goals.
Uterine Artery Embolization: Step-by-Step Guide
Preparation: Doctors review the patient’s history, order blood tests, a pregnancy test (UFE is a no-go if the patient is pregnant), and a pelvic MRI or ultrasound to map fibroids and blood vessels. A brief fast is prescribed and instructions on medications are given.
Anesthesia and Access: The patient may be sedated mildly or given local anesthesia. A small incision is made either in the radial or femoral artery to insert a thin sheath.
Catheter Placement: Through real-time X-ray (fluoroscopy), a flexible catheter is inserted into the blood vessel to the uterine arteries providing blood flow to the fibroids. This will be confirmed using dye.
Embolization: In a sense, embolization has the opposite intended effect of angioplasty. Angioplasties aim to widen arteries and increase blood flow, embolizations aim to reduce/control blood flow and ‘starve’ certain growths or organs, so they can shrink. Small particles are delivered into the artery via a microcatheter. This leads to reduced blood flow to fibroids and their shrinkage. The procedure is done on both sides at once.
Completion and Recovery: Post-procedure X rays check results, the catheter is removed, and the access site sealed. Patients rest for 4-6 hours before being discharged, controlling pain through medication.
Most patients report dramatic pain relief within days to weeks, as the fibroids shrink. However, it is important to remember that shrinkage is not immediate and the time period could vary depending on the extent of growth and other patient-specific factors.
Advances in Uterine Fibroid Embolization Procedural Technology
Embolizing agents: The kind of agents used for embolization are evolving — calibrated spherical microspheres, and new generations of particles like calibrated hydrogel microspheres and gelatin-based fully resorbable particles (that are biodegradable) have become the gold standard. Their mechanism is now better understood and hence, outcomes more predictable.
Approach and patient convenience: The transradial approach and improved local anesthesia or nerve blocks have minimized the complications related to the entry site and allowed many UFE procedures to be outpatient.
Imaging and planning: pelvic MRI has become the preferred modality for mapping fibroid size, number, location, and for planning and predicting response. MRIs also detect coexisting conditions that an ultrasound may miss — like adenomyosis or suspicious masses — that could alter or contraindicate embolization. Intra‑procedural digital subtraction angiography remains essential.
Pain management protocols: multimodal analgesia, peri‑procedural nerve blocks and optimized post‑op regimens have shortened hospital stay and improved patient experience.
Recovery and Rehabilitation After Uterine Artery Embolization
Immediate hours
After the procedure the patient will spend several hours in recovery where nurses monitor vital signs and manage pain with medicines. Cramping similar to strong period pain, nausea, and sometimes a low‑grade fever can be expected; these are part of the normal post‑embolisation response. Prescribed pain medication, a heating pad, and rest are recommended during this time.
First week
The cramping and pain will be more severe during the first 48–72 hours and should then ease up. Minor bleeding or dark discharge may occur. Plenty of fluids, sticking to smaller food portions, refraining from lifting anything heavy, and lots of rest. Doctors don’t usually recommend sex during this time.
Weeks 2-6
Energy recovers slowly, but most people can go back to their office or light jobs within 3 to 7 days, while more physically demanding occupations take between 2 and 4 weeks based on how painful it is. Strenuous physical activity and lifting varies by prior conditioning (athletes obviously have a higher baseline), but it’s recommended to be very conservative with this to promote full healing. It’s a good idea to check with doctors about sex, to ensure it does not become an uncomfortable painful affair.
Post-procedure follow-up and long-term
The outpatient evaluation after 4 to 12 weeks checks symptoms and recovery progress. An ultrasound or MRI may be required after 3 to 6 months to assess fibroid reduction. Symptoms tend to start improving within a few weeks, progressing for months as the fibroids gradually shrink. If there was anemia before, supplements may be prescribed and the improvement is visible via less bleeding. However, blood counts are required to measure this quantifiably.
Red flags
Increasing fever above 38°C, heavy vaginal bleeding soaking a pad every hour, severe uncontrolled pain, foul‑smelling discharge, difficulty urinating, or signs of infection require prompt medical review. It’s crucial to not ‘wait and see’ here.
Benefits of Uterine Fibroid Embolization
- Symptom relief: The UFE procedure helps alleviate heavy menstrual periods and pelvic pressure in a majority of cases, usually within weeks, thus increasing energy levels and the overall quality of daily life. It’s very hard going about work, socializing or just about anything when in constant discomfort; the mental toll is rather underemphasized.
- Preservation of uterus: Unlike hysterectomy, where one has to remove the uterus entirely, the UFE procedure leaves it intact. For those interested, reproduction is still a possibility.
- Minimally invasive: The procedure uses a small puncture in the wrist or groin, so there’s less blood loss, no large incision, and usually a faster recovery than open surgery.
- Shorter hospital stay and faster return: The majority of patients go home on the same day or the next day and resume their activities at a relatively quicker pace, compared to surgery.
- Lower surgical risk for some patients: For women with other health issues that make surgery risky, UFE is a safer alternative with fewer anesthesia and operative complications.
- Durable results with symptom improvement: Most patients benefit from the procedure with a reliable decrease in symptoms; there’s no need for repeated intervention in most cases.
Comparison of Uterine Artery Embolization, Myomectomy & Hysterectomy
| Comparison | Uterine Artery Embolization | Myomectomy | Hysterectomy |
|---|---|---|---|
| What it does | Blocks the blood supply to fibroids so they shrink over weeks–months. | Surgically removes fibroids while preserving the uterus (hysteroscopic, laparoscopic/robotic, or open). | Removes the uterus (sometimes with ovaries/tubes), permanently eliminates fibroids. |
| Best for | Women who want to keep their uterus, need relief from heavy bleeding or pressure, or are at higher surgical risk. | Women who strongly desire future pregnancy or when fibroid distorts the uterine cavity. | Women who do not want future pregnancy and desire definitive treatment. |
| Hospital stay & recovery | Often same‑day discharge or overnight; light activity in 3–7 days, fuller activity in 2–4 weeks. | Minimally invasive: 1–2 weeks; open abdominal: 4–6 weeks. | Vaginal or laparoscopic: 2–6 weeks; open: 4–8 weeks. |
| Effect on fertility | May reduce fertility; pregnancy is possible but may carry higher obstetric risks than myomectomy. | Preferred for fertility preservation; generally better pregnancy outcomes when cavity‑distorting fibroids are removed. | Fertility permanently eliminated. |
| Symptom relief durability | Good symptom relief for most; a minority need repeat procedures or later surgery. | Good symptom control but fibroids can recur (recurrence rates vary). | Permanent and complete resolution of fibroid symptoms. |
| Main risks | Post‑embolisation pain/fever, infection (rare), possible ovarian dysfunction, small chance of needing hysterectomy. | Bleeding, infection, adhesions, recurrence; surgical/anesthesia risks (higher with open surgery). | Surgical risks (bleeding, infection), longer recovery for open surgery; if ovaries removed, causes immediate menopause and related effects. |
Risks and Complications of UFE
Any procedure comes with some effects on the body — navigating the recovery process becomes less taxing, when one is aware of these potential complications:
Common short‑term effects: Many patients experience the “post‑embolisation syndrome” — cramping pelvic pain, low‑grade fever, nausea, and fatigue for 1–5 days; these are usually managed with pain medicines and rest. More a symptom than risk, but worth expecting, so there’s no panic. Post procedure recovery can be an emotional and anxious time for many patients.
Risks associated with the access site: The small puncture in the wrist or groin can bleed, bruise, or rarely form a hematoma or infection; even if this were to happen, this is easily treatable.
Infection and serious complications: Rarely, infection of the uterus or retained tissue can occur and may need antibiotics. In very rare cases, this may escalate into a surgical removal of the uterus. Non-target embolization: Embolization requires a delicate precision. Very rarely, embolic particles may travel to non-target organs nearby and cause unintended damage. Experienced interventional radiologists rarely run into this situation, because of years of refined technique.
Ovarian dysfunction and menopause: UFE may decrease ovarian blood supply, leading to temporary or even permanent ovarian insufficiency (menopause occurring earlier than normal), especially in older patients.
Fertility and pregnancy risks: Pregnancy after UFE is possible but may have higher risks such as miscarriage, preterm birth, placental problems. These potential complications are slighter higher when compared to myomectomy. Discussing family plans in advance definitely helps.
Additional treatment needed: Rare, but not entirely non-existent. Some women do experience recurrent symptoms and require further embolization or in very select cases, surgery.