

Prostate Artery Embolisation
 Home
Home- Prostate Artery Embolisation

Medically Reviewed By Dr. Karan Anandpara Updated on February 23, 2026
Prostate artery embolisation (also known as prostate artery embolization) is a minimally invasive procedure indicated primarily for the treatment of benign prostatic hyperplasia (BPH). This is a condition also referred to as ‘enlarged prostate’, typically in men over the age of 50. A non-cancerous (benign) growth of the prostate causes the gland to press on the urethra, causing many lower urinary tract symptoms (LUTS). Some of these include a frequent or urgent need to urinate, dribbling after urinating or trouble starting urination.
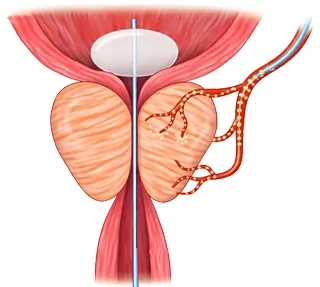
Prostate artery embolisation is performed by the delivery of small particles through a catheter to block blood flow to the prostate, thereby encouraging a reduction in size. It is considered an alternative to surgical interventions like TURP (Transurethral Resection of the Prostate).
Conditions Treated by Prostate Artery Embolisation
As explained, PAE is almost exclusively used to treat Benign Prostatic Hyperplasia (Enlarged Prostate), a condition in men over the age of 50 that can be non-fatal, but very disruptive to work, sleep, travel and just daily comfort. While not a physical aspect, BPH can also be a somewhat socially difficult condition that causes emotional stress due to its private and delicate nature.
Hormonal changes with age drive prostate cell growth around the urethra, not linked to prostate cancer. Symptoms worsen gradually if untreated, risking infections, bladder stones, or retention.
Beyond LUTS, however, PAE excels in more challenging BPH scenarios: acute or chronic retention of urine — when one cannot pass urine, but the bladder function remains reasonable. Here PAE can help avoid permanent damage. Another such condition is prostatic hematuria — painless blood in the urine, due to prostate bleeding. There are other conditions and patient profiles where surgery may be considered too risky.
Examples of these would be elderly patients with heart issues, diabetes or lung problems, bleeding disorders (coagulopathy). Apart from these, it’s a viable option for patients who simply refuse to go through a surgical procedure like TURP. This unwillingness could stem from a fear of the side/after effects, recovery time, or any sort of past surgical trauma. PAE simply cuts off overfed prostate arteries to shrink the gland safely, preserving all sexual function. Recovery times are quick, and it can be a game changer when meds fail and surgery isn’t ideal.
Indications to Perform Prostate Artery Embolisation
Normally, medications are the first line of intervention to address BPH. If LUTS won’t go away, despite the use of alpha-blockers, 5-alpha-reductase inhibitors and other medicines, PAE is considered.
While there’s no qualifying size, as such, doctors recommend PAE for bigger prostates over 80 cm³ (measured by ultrasound or MRI). There’s no real size cap, also making it a great option for ‘super sized’ cases, where surgery is difficult. PAE also stands out as an option for patients who require a catheter to drain the bladder, due to retention., Additionally, it’s highly recommended for those who’d like to keep their sex life intact (functions like erection and ejaculation). Surgeries can disrupt that.
As mentioned above, it’s also ideal for older hypertensive patients, those with cardiovascular issues or diabetes, and those at a risk of bleeding. PAE is also prioritized in patients with general weakness, as surgery can be quite physically exhaustive.
Before greenlighting PAE, a urologist will first aim to rule out other potential causes of LUTS such as urethral stricture or neurogenic bladder, possibly through less-invasive means like examinations or cystoscopy. If a prostate is less than 60cm³, PAE is not recommended. If a CT angiogram reveals severe atherosclerosis, it is also not recommended.
Step-by-Step Guide to Prostate Artery Embolisation
It is a rapid, outpatient procedure performed under local anaesthesia. Here’s how it goes, step-by-step:
Access the femoral/radial artery under local anesthesia; advance the catheter to internal iliac via fluoroscopy/CBCT
The doctor numbs a small spot in the patient’s groin (femoral) or wrist (radial) artery. After this, a thin, flexible tube (catheter) is threaded up to the pelvic arteries. Procedural guidance is provided by a live X-Ray (fluoroscopy) and 3D imaging (CBCT). Think of this like a GPS for the blood vessels. This is typically painless and safe.
Identify/select prostatic arteries (PAs) with CBCT/DSA; inject vasodilator to ease navigation
Special scans highlight the miniscule prostate feeding arteries; a mild relaxing drug is jetted in to open them up, thus facilitating smooth navigating without any spasms.
Superselect PA branches beyond collaterals (to bladder/rectum/penis); embolize proximally first to near-stasis with microspheres (250-500 μm)
The catheter tip is designed to target safe branches, not near to any connections to the bladder, rectum or penis. First, small bead-like objects called microspheres block the main artery, until blood flow is halted almost completely.
Advance microcatheter distally into parenchyma; embolize anteromedial then posterolateral branches to stasis, "pack-back" while retracting
A smaller catheter goes deep into prostate tissues; beads plug the front–inner, then back–outer sections until blood flow stops, pulling back while adding more for full coverage, like sealing every path.
Repeat bilaterally; procedure lasts 1-4 hours outpatient
Both sides of the prostate get treated, and the procedure is complete within 1-4 hours, depending on the complexity. Often, the patient is discharged the same day.
Advanced Techniques in Prostate Artery Embolisation
Compared to basic PAE, there are more sophisticated variations that are even more effective in shrinking an enlarged prostate. One of these is PErFecTED (Proximal Embolisation First, Then Distal). Here, doctors first block the main artery close to its start (proximal), thereby cutting off big blood supply. Then, they go deeper into prostate tissue for targeted embolisation. This double step improves results — better symptom scores (IPPS drops) and stronger urine flow (Qmax), compared to basic PAE.
There are other updates such as CBCT, which facilitates a 3D plot of tricky vessels, vasodilaters to reduce spasms. This makes it easier for the catheter to pass varied diameters of microspheres (100-500µ), which facilitates blocking without leakage, and radial access, which utilizes the wrist instead of the groin to reduce exposure and contrast dye by up to 50%. These refinements mean fewer complications, faster treatments and tailored options for complex cases.
Benefits of Prostate Artery Embolisation
PAE offers incredible relief from BPH, but with fewer risks and ‘downsides’ than traditional surgery. It reduces the IPPS (International Prostate Symptom Score) by 9 to 21 points. The IPPS is a standardized measure of urinary woes like frequency and weak flow. These gains match up to the short-term wins from TURP, but without the invasive risks.
Many argue that the greatest advantage of PAE is the preservation of sexual function. TURP often causes retrograde ejaculation (semen backs into the bladder) in 65-70% of men and erection issues. TURP also has a 4-6 week downtime, with hospital stays up to 3 nights. PAE allows a patient to resume light activities within 2-3 days. Also, major complications, especially risk of infection or bleeding are very rare, at just 2.5%.
PAE definitely beats medication for lasting LUTS. The prostate gland typically shrinks by 20-30%; over the course of 3-6 months, a patient's PSA level will decrease by 20-30%. PAE is also a repeatable procedure, with few added risks if symptoms begin to return. In terms of quality of life, PAE really stands out. Quick recovery, less scarring and no impact on sexual function, which is a very important aspect of life.
Reference - PubMed Central – Prostate Artery Embolisation as Minimally Invasive Treatment for Benign Prostatic Hyperplasia: An Updated Systematic Review.
Risks and Complications of Prostate Artery Embolisation
As explained above, PAE is a very safe procedure. It is a procedure nonetheless, and that means it does come with a few risks — mostly mild and short-lived.
Common minor issues (affecting 10-30% temporarily):
Post embolisation syndrome hits during the first few days. This may manifest as mild pelvic pain or burning while urinating, fever and fatigue. Not unlike a flu that will resolve on its own within a few days. UTIs (Urinary Tract Infections) affecting 2-8% of patients can also be managed. While temporary, patients may notice traces of blood in urine or semen. This is commonly referred to as hematuria or hematospermia, respectively. These too resolve themselves within 1-2 weeks without cause for concern.
Rare major complications (<5%):
Nontarget embolisation, such as bead drifting to the bladder, penis or rectum, is under 1%. This could temporary ischemia (reduced blood flow) or in very rare cases, necrosis (tissue damage). Experts use imaging to avoid this. Acute retention or prostatitis might require a short catheter or meds, but resolves quickly.
Unlike some surgeries, there is NO known risk of incontinence or impotence. The amount of radiation used is the equivalent of two to three CT scans. Major complications are nowhere near as common as TURP. Most men sail through with excellent outcomes.
Recovery and Rehab
The recovery process following PAE is generally quite straightforward and devoid of complications. Regular activities may be resumed within a few days, without an elongated hospital stay. Relieving symptoms, like improved urination and reduced need for urgent bathroom breaks, gradually occur as the prostate gland shrinks in size.
For the first, as mentioned above, there might be some mild discomfort in the pelvis, fatigue and some changes in urination. These are normal and can be dealt with through good hydration (2-3 litres a day). Sometimes, analgesics like Ibuprofen are recommended. Heavy lifting and very core intensive activities (any sort of squeezing and ‘try hard’) are ideally avoided. A catheter, if needed, will come out in 24-48 hours.
Follow-ups matter! A doctor will typically check symptom scores (IPSS for urinary issues and QoL for quality of life) at 1-3 months. An ultrasound or MRI is taken at 1-6 months to measure prostate shrinkage. Antibiotics may be prescribed for UTI. Most patients feel around 50-70% better by one month. By three months, life is usually completely back on track. Improved sleep scores are also an indicator of this.
BPH and Prostate Artery Embolisation in India
BPH affects about 50% of Indian men, by the age of 60. Prevalence rises from 25% at 40-49 years to 50% at 70-79 years.
PAE adoption is growing in India, especially in urban areas. A short-term 2024 study of 25 patients found short-term effectiveness aligning with global IPSS reductions of 14-30% and 22-28% volume shrinkage. Success rates hit 85-93% at 12 months with very low complications.
Reference - PubMed Central – Prostate Artery Embolisation: An Initial Experience from an Indian Perspective.
Picking the right hospital/doctor:
Always look for interventional radiologists who’ve done hundreds of PAEs — they are comfortable with tricky prostate artery maps, and use advanced CBCT imaging to avoid potential risks like beads going astray.
Opt for team care: A radiologist and urologist, for a complete evaluation.
Questions to ask your doctor:
- Does my profile make PAE ideal over TURP?
- What symptom improvements can I expect at 3-6 months?
- What are the risks specific to me?
- How will this affect sexual function?
- When can I resume having sex?
- Any specific activity restrictions? If so, why?
- How many PAEs have you done?
- What is the follow-up schedule?
Frequently Asked Questions
What is prostate artery embolisation (PAE)?
Prostate artery embolisation (PAE) is a minimally invasive procedure used to treat an enlarged prostate by blocking the blood supply to the prostate, causing it to shrink and improving urinary symptoms.
Who is a candidate for prostate artery embolisation?
Men with benign prostatic hyperplasia who have moderate to severe urinary symptoms and wish to avoid surgery may be candidates for prostate artery embolisation. Suitability is determined after evaluation by an interventional radiologist and urologist.
How long does prostate artery embolisation take?
The procedure usually takes about 1 to 2 hours and is performed under local anesthesia with imaging guidance, so most patients remain awake and comfortable.
What is the recovery time after PAE?
Most patients can go home the same day or the next day and resume normal activities within a few days, which is significantly faster than recovery from surgery.
Is prostate artery embolisation safe?
PAE is considered a safe minimally invasive procedure with a low risk of complications when performed by experienced interventional radiologists, though every procedure carries some risks discussed during consultation.
How effective is prostate artery embolisation?
Clinical studies, including systematic reviews, have shown that PAE can significantly improve urinary symptoms and quality of life in many patients with an enlarged prostate.