

Pelvic Congestion Syndrome
 Home
Home- Pelvic Congestion Syndrome

Medically Reviewed By Dr. Karan Anandpara Updated on June 01, 2026
It is like varicose veins in the pelvis — dilated, twisted veins that pool blood due to faulty valves, causing ongoing ache or heaviness. The condition is also referred to as pelvic venous insufficiency. mainly hits women aged 20-45 who've had multiple pregnancies, as hormonal shifts (like estrogen surges) and pregnancy pressure weaken vein valves, leading to backward blood flow. The condition can be persistent and aggravates as the day progresses, before getting a period, during sex or even prolonged standing. It can also result in bloating and an increased urge to urinate. While not always ‘critical’, pelvic congestion syndrome can massively disrupt life quality — degrading the ability to get sound sleep, work productively, socialize and have a healthy sex life. Symptoms can mimic endometriosis; the overlap and resulting confusion leaves PCS undiagnosed for years.
Globally, PCS explains 10-30% of chronic pelvic pain conditions (40% of gynaecologist visits relate to this). In India, the prevalence varies from 12-33%, primarily showing in women with multiple pregnancies (multiparous). Early diagnosis via ultrasound or embolization brings 75-90% relief.
Causes of Pelvic Congestion Syndrome
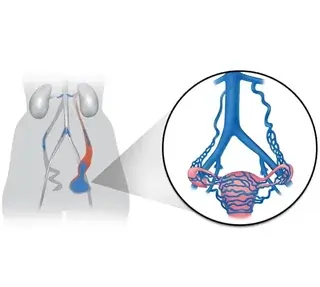
PCS happens when veins deep in the pelvis like the ovarian and iliac veins don’t work properly — they let blood flow backward, instead of up to the heart. This is the same problem mechanism as varicose veins. Faulty valves inside these veins fail to stop this backflow, causing the veins to stretch, twist into varices (like varicose veins in the leg) and trap blood that presses on nerves, sparking the ache. Factors associated with PCS:
Pressure from pregnancy: Each pregnancy stretches pelvic veins and ramps up blood volume by 50%, weakening vein walls — the effect is exacerbated if the patient has had two or more babies. Due to the growth of the uterus, there is pressure on veins, and the nutcracker syndrome (left renal vein pressure) can make things worse.
Hormonal shifts: Increase in estrogen softens/weakens vein walls during core reproductive years (20-45), making them floppy and prone to reflux. Progesterone fluctuations before periods worsen this.
Other factors: Genetic predisposition (family history of venous problems), obesity (excess abdominal pressure), or standing jobs. There’s no single ‘aha’ cause — it’s usually a combination of factors that can even be confused with IBS or fibroids; this can get tricky. It’s important to visit a doctor early and get an ultrasound, to prevent the issues from getting worse.
Risk Factors for Pelvic Congestion Syndrome
Women between 20 and 45 years of age, particularly those who have had two or more pregnancies, are most prone to PCS due to their enlarged pelvic veins and increased blood volume that stretches them repeatedly.
Main Risk Categories
- Reproductive history: Multiple pregnancies increase pressure on ovarian veins from the growing uterus, making reflux more likely — up to 30% higher risk after 3+ pregnancies.
- Anatomical factors: A retroverted (tilted-back) uterus traps blood flow by creating pockets; polycystic ovaries add hormonal chaos; "fullness" in leg veins signals broader varicose tendencies.
- Hormonal influence: Being premenopausal means an increased estrogen production — this relaxes vein walls, and any further imbalances only worsen the dysfunction.
- Lifestyle links: Obesity (this is one of the broadest health risks), long hours standing, or a family history of venous issues amplify odds. In India, multiparous women in urban areas report higher rates due to delayed diagnosis — this tends to happen due to the mimicking effect of PCS (very similar to IBS, endometriosis and fibrosis). Spotting the differences early via an ultrasound can be crucial to guiding relief.
Diagnosis for Pelvic Congestion Syndrome
Identifying PCS begins with tracking and listening to the body’s signals — ongoing pelvic ache worsened by sex, standing, or periods. Then, the process of ruling out mimics like fibroids or endometriosis begins.
First Steps
Doctors review symptoms, family history, and do a pelvic exam (though veins shrink when lying down, so it may miss clues). Blood tests check hormones or inflammation.
Key Imaging Tests
Ultrasound (with Doppler): Non-invasive starter test; it’s conducted in a standing position, which can show dilated veins (>5-10mm) and backward blood flow (reflux). A transvaginal version zooms inside.
MRI or CT scan: These scans allow visualizing of twisted veins and exclude tumors; MRI venography serves as the most informative non-invasive investigation.
Gold Standard: Venography: If something suspicious is found, this is the next step. A catheter is inserted into the groin vein with dye injection; an X-ray shows precise sites of reflux. This usually takes a patient directly to treatment such as embolization.
Laparoscopy (if needed): If a venography isn’t satisfying, this is a more guaranteed line of imaging. A tiny camera checks inside the pelvis for varices, hoping to capture detail that the imaging couldn’t.
Doctors like to avoid separate catheterization procedures for diagnosis and treatment, wherever possible, as these can be inconvenient and even painful for the patient.
Symptoms that distinguish Pelvic Congestion Syndrome
What makes PCS truly different from other causes of pelvic discomfort like IBS, fibroids or endometriosis? This has to do with the particular symptom pattern tied to vein congestion. First and foremost, the nature of pain.
Classic PCS signs
Chronic dull ache in the lower pelvis or lower back, lasting over 6 months, that worsens by late afternoon (after standing/walking) or pre-period — eases when lying down. This is the first alarm.
Pain during/after sex (post-coital ache), unlike sharp endometriosis pain. PCS pain is dull and aching. Endometriosis pain is very sharp and stabbing. The pain also varies by position.
Differentiating clues
Visible leg/varicose veins or vulvar swelling, hinting at venous issues (rare in gynaecology disorders). Feeling of pelvic fullness/pressure, like a heavy dragging, plus bloating, bladder urgency, or hemorrhoids — worse with lifting and a history of pregnancy. No alarming signs like fever, weight loss, or any other sign of infection/malignancy (cancer).
If these signs fit, and the patient is in the 20-45 age group with multiple pregnancies, it’s worth asking for a Doppler ultrasound — PCS explains 10-30% of stubborn cases that other imaging modalities may miss.
Treatment for Pelvic Congestion Syndrome
Step 1: Conservative Relief
This stage is focused on changing up some habits and medications. Lying down when the pain flares or the use of compression stockings can help. NSAIDS like Ibuprofen can offer reasonably quick relief.
Anti-inflammatory meds calm vein irritation; avoiding longer periods of standing helps. If the pain isn’t too debilitating, these measures can carry on for a while.
Step 2: Hormonal Therapies
If the pains become debilitating, another line of medications are considered. These suppress estrogen's vein-weakening effects:
Progestins and birth control pills relieve mild symptoms, decreasing pain by 50 to 70%. Gonadotropin-releasing hormone agonists induce artificial menopause, preventing blood accumulation; these work for 3 to 6 months. These are all great starters, but not curative. They simply manage symptoms to make daily life more convenient. There are classic side-effects like hot flushes and mood swings, as a result of some medications.
Step 3: Ovarian Vein Embolization (OVE) - The gold standard
This is the next step towards ‘solving’ the problem. A minimally invasive outpatient procedure where an interventional radiologist inserts a catheter through the femoral vein into the abnormal ovarian veins and blocks these veins using either coils (small springs) or a sclerosing agent (foam irritant). This ensures proper blood flow, resulting in a 75-90% cure rate (with more than 80% pain reduction). OVE is typically much safer than surgery, with most returning to normal life within 1 or 2 days.
Step 4: Uncommon Surgical Solutions
If embolization is unsuccessful: vein ligation (laparoscopic tie-off) or hysterectomy (for severe cases only) may be considered. These come with higher risks and recovery times; they’re used in less than 10% of cases now.
Benefits of Pelvic Congestion Syndrome Treatment
Treatment for PCS offers a huge leap in the quality of life. OVE changes the lives of thousands of women, across the globe. It fixes the root issue without surgery or much downtime.
Key wins:
- Pain relief: 75-85% report remarkable improvement (typically 80%+ reduction) in just days; research indicates that effects last up to 80-90% in 1-2 years. For most, this is the biggest win.
- Low recurrence: Just 5-10% recurrence since blocked veins stay sealed.
- Life quality: Patients return to work within 1-2 days and have sex within 7-8 days; they report an increase in energy levels, sleep quality, libido and bloating — many call it ‘life changing’, understandably.
Hormonal therapy benefits:
Pills or injections calm symptoms in 50-70% of patients, in the short-term, by taming estrogen. A perfect ‘trial run’ before considering OVE.
Both skip the risks of hysterectomy, and preserve fertility.
Recovery and Rehabilitation
Recovery following OVE in cases of PCS is usually quick and uneventful, allowing patients to return to their normal activities rapidly.
Immediate post-procedure (Day 1)
Patients rest in the clinic/hospital for 4-6 hours with groin pressure to prevent bleeding — mild cramping or nausea is common but fades quickly. They head home the same day; most feel better by the evening. Painkillers are recommended; ice packs can soothe the groin area.
Short-term recovery (Days 2-7)
Patients engage in light activity (walks and desk work) after 1-2 days, normal life typically resumes within 1 week. They’re recommended to skip heavy lifting (>5 kgs), full bathing or sex for a week. This is to allow the coils to settle. If there’s leg swelling, compression stockings can help. By this stage the pain has already reduced by 50-80%.
Longer-term rehab (Weeks 2+)
Pain relief gradually improves after 1-3 months as the veins form new pathways. Pelvic floor PT (kegels, stretches) strengthens muscles weakened from chronic strain, preventing bladder issues or prolapse. Ideally, these exercises are done 2-3 times a week. Post PT, a longer-term pelvic floor-focused exercise regimen is definitely beneficial.