

Carotid Artery Stenting
 Home
Home- Carotid Artery Stenting

Medically Reviewed By Dr. Antariksh Vijan Updated on May 12, 2026
Carotid artery stenting (CAS) is a procedure used to address severe stenosis of the carotid arteries located in the neck. This narrowing is due to plaque formation from cholesterol and fat accumulation. The carotid arteries provide oxygen-filled blood to the brain; if they get blocked, there is an increased risk of strokes through obstruction or clot migration up the vessel. CAS is a minimally invasive option that offers a much safer alternative to open-neck surgery (enarterectomy), especially for higher-risk patients with heart issues or prior radiation (often for treating issues like head, neck or thyroid tumours).
The procedure is performed via a small groin puncture under local anaesthesia, doctors thread a catheter to the blockage, deploy a mesh stent to open the artery up, and use filters to catch the debris (more procedural details are provided below). The procedure has a remarkable success rate, with one study from 2022-23 showing a 100% procedural success rate. 79.5% of patients fully recovered with no significant restenosis on follow ups.
Conditions treated by Carotid Artery Stenting
Carotid artery stenting primarily treats the condition of carotid artery stenosis (carotid artery disease). The arteries become narrow due to the build up of plaque — made of cholesterol, fats, calcium and other debris. These are extremely vital arteries that carry oxygen-filled blood from the heart to the brain. Severe blockages (over 50-70%) can cut off that flow and also risk clots travelling upstream, severely increasing the risk of a stroke or even a ‘mini-stroke’, medically called a transient ischemic attack (TIA).
Carotid artery stenting is used for two key groups:
- Patients with symptoms: People who’ve recently had TIA (weakness, visual problems, speech problems) or a small stroke resulting from 50-99% stenosis of the artery. Early treatment reduces the chances of another stroke.
- Asymptomatic patients: No symptoms, but scans show 70-99% blockages. Here, the procedure is preventive, especially for those at high surgical risk.
Beyond these broad categories, CAS already addresses restenosis after carotid endarterectomy surgery, complicated cases such as high-neck lesions, history of radiation damage (fibrosis), heart/lung issues making open surgery risky, or a blocked artery on the opposite side (contralateral occlusion).
In a generalized sense, think of plaque like rust or hair balls clogging a pipe. CAS deploys a mesh-tube — the stent — to expand it safely, without any cutting. A highly viable option for high-risk patients where traditional surgery comes with too many complications.
Step-by-step Guide to Carotid Artery Stenting
The carotid artery stenting procedure is fast and minimally invasive, performed in a cath lab. It typically takes about 1-2 hours and is performed under local anesthesia, not general anesthesia. A patient will remain awake and coherent throughout the procedure.
- Prep and access: The first step involves creating a small incision in the groin (femoral artery) or wrist (radial artery), through which a catheter will be inserted; this will navigate its way to the carotid artery via fluoroscopic (live X-ray) guidance.
- Brain protection: A miniature filter or balloon is placed downstream of the blockage to ensure that any plaque fragments don’t travel toward the brain.
- Map the blockage: Contrast dye is injected to light up the artery on X-ray, showing exactly where the plaque is.
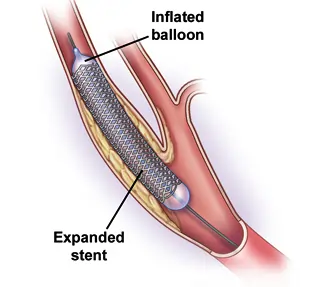
- Open and stent: Initially, a small balloon inflates briefly (predilation) to flatten the plaque. Then, a mesh stent is implanted — this acts like a tiny spring that keeps the artery expanded. Occasionally, another balloon may be used for we may use another balloon to perform post-dilation.
- Assessment and closure: More dye confirms optimal blood flow. Once done, all devices are withdrawn, the puncture site is sealed, and the patient’s condition is monitored for several hours before evaluating for discharge or overnight stay at the hospital.
Advancements and New Techniques in Carotid Artery Stenting
New carotid artery stenting technologies ensure greater safety and precision, thereby minimizing the risks of stroke occurrence. Below is a list of things worth looking into, if eligible for the surgery:
- Dual-layer micromesh stents: Newer stents have two layers with tiny pores to trap plaque debris, cutting brain emboli better than older single-layer ones. They promote healing and have high success rates in protecting against restenosis.
- Flow reversal protection: Rather than using filters, the process involves reversal of the blood flow within the vessel (E.g., TCAR approach). It is not possible for plaque fragments to reach the brain due to this approach. This is especially suitable for patients with complicated anatomy; an incision is made in the neck for the procedure.
- Radial access: While not an ‘advancement’, radial access is trickier than the classic femoral access. Trials show 100% success rates, with fewer site issues.
- Robotic technology: Robot-assisted stenting allows for enhanced precision of the surgery, reduces radiation levels and minimizes physician fatigue — an under-discussed but extremely valuable aspect for surgical success. This is emerging in many advanced centers for complex cases.
Who is a Candidate for Carotid Artery Stenting?
Carotid Artery Stenting (CAS) is typically diagnosed following reports of dizziness, vision changes, weakness, impaired motor response or a ‘whooshing’ sound in the neck heard through a stethoscope. In general, the process of diagnosis is sparked by stroke suspicion/TIA workups. First Carotid ultrasound, then, CT angiography and finally cerebral angiography to confirm CAS.
Doctors will suggest a CAS in the following scenarios:
- Symptomatic Stenosis (50-99%): If the patient has suffered a stroke, TIA (with symptoms such as weakness, difficulty in speech and loss of vision), or any warning sign due to ≥50-70% blockage in arteries. CAS quickly restores blood flow dramatically reducing the risk of a repeat event, especially within weeks.
- Asymptomatic Severe Stenosis (≥70%): There are no symptoms; however, ultrasound or angiography reveals serious narrowing of arteries. It is preventive if the patient is healthy enough, to reduce long-term stroke odds.
- High Surgical Risk: Conditions such as heart failure, poor pulmonary function, recent myocardial infarction (heart attack), or a low ejection fraction (EF) make neck surgery dangerous. CAS avoids big cuts.
- Prior Neck Issues: Prior radiation (fibrosis), unsuccessful endarterectomy (restenosis), proximal lesions, or occlusion in the opposite artery.
Doctors weigh scans, symptoms, age and overall health — often starting meds like aspirin/statins first. Guidelines favour CAS for average/lower risk profiles with <6% complication odds. Even if a patient has a higher surgical risk profile, their CAS risk profile can be lower.
Risks and Complications of Carotid Artery Stenting
CAS is generally a safe procedure, with extremely good success rates and patient outcomes. But, it does carry some risks, like any procedure. However, these are quite low (<5%). A good doctor will typically go over these risks with a patient, and weigh them against the potential benefits before taking a call to proceed.
Immediate risks (during/soon after):
- Stroke or TIA (3-5%): Microembolism caused by fragments of plaque despite use of filter; most of these get resolved quickly.
- Groin-site bruising/blood loss: Common, but very minor. Very rare cases of hematoma requiring draining.
- Heart arrhythmia: Transient bradycardia (slow heart rate) due to stretching of the artery; managed with medications.
Long-Term Complications (weeks to years):
- Restenosis (5-10%): Narrowing of the artery again; tracked using ultrasound. Rarely needs restenting.
- Stent thrombosis: Formation of clot in the stent (below 1%, with the use of anti-clotting agents like aspirin and clopidogrel).
- Others: Nerve irritation (hoarseness, rare), kidney strain from dye (pre-hydrate helps).
Benefits of Carotid Artery Stenting
The greatest benefit of CAS is that it is a highly effective and accessible alternative to surgery (endarterectomy). Patients of varied risk profiles can benefit from this, as a method of stroke prevention.
Immediate procedure perks:
Minimally invasive: Just a tiny groin or wrist puncture — no large neck cut, less pain, and no general anesthesia (the patient is awake but relaxed).
Convenient: It takes 1 to 2 hours, and you can get out of the hospital the following day (staying 1-2 days in hospital).
Benefits for Recovery:
Rapid recovery: Start with gentle exercises within days, return to driving or work within a week, perfect if surgery is not an option.
Initial safety considerations: No problems with neck nerves/irritation; suits patients with heart or lung conditions or those with radiation scars.
Long-term wins:
Effective stroke protection: Opens artery ≥90% of time, slashing recurrent stroke risk (similar to surgery in trials).
Durable results: Stent keeps flow steady; India data shows 80%+ full recovery, low re-narrowing.
Limitations of Carotid Artery Stenting
While CAS matches surgery (carotid endarterectomy or CEA) in long-term stroke prevention, CEA excels in a few areas where CAS falls short, based on trials like ACST-2, CREST, and ICSS.
It’s important to understand these limitations and differences, so patients and doctors can make an informed decision.
The biggest difference is that CAS poses a higher 30-day risk of any stroke (1.6x more than CEA), especially non-disabling strokes. Additionally, CEA’s direct removal of plaque lowers the odds of emboli.
Certain anatomies are also easier for CEA to handle — tortuous vessels, heavy calcification, or high aortic arch plaque. In the case of complex anatomies, CAS struggles with wire navigation or stent delivery.
CEA also avoids lifelong dual antiplatelets (which is a CAS requirement). While not extremely worrisome, antiplatelet meds do come with their own side effects — bleeding risks initially, and then stomach issues, nausea, dizziness, headache and diarrhea. In very rare cases (<2%), there is a chance of intracranial hemorrhage, blood in stools, and low platelets.
However, in most cases, the benefits significantly outweigh the risks. CEA is preferred for low-risk and symptomatic cases under 70. CAS for higher-risk profiles.
Recovery and Rehab
Recovery from carotid artery stenting (CAS) is typically smooth and quick, with most patients resuming normal life in days. Here’s a stage-wise breakdown:
Immediately after procedure (24 hours):
Observation in the hospital to monitor blood pressure, heart rate, and neurological functions to look for any complications such as stroke.
Patients are asked to lie flat for 4-6 hours to seal the groin area; some pain is expected. Discharged within 24 hours if all is well.
First week (home):
Bed rest, no strenuous activities; short walks are encouraged to avoid clotting.
Dual antiplatelet therapy with aspirin and clopidogrel prescribed, with immediate medical attention needed if bleeding, headache, or weakness persists. Here, it’s important to be vigilant and pay attention to smaller sensations. Feelings of ‘wooziness’ (mild dizziness and some disorientation) and fatigue aren’t to be ignored.
Weeks 2-4 (full recovery):
Resume driving/light work after 1 week; avoid neck strain (switching to comfortable pillows can help avoid spasms or any odd strains). Follow-up ultrasound checks stent functionality. Transition to aspirin alone; blood pressure/cholesterol is managed with meds.
Prolonged rehabilitation (long term):
Healthy heart practices: The usual — dropping smoking and alcohol habits, reevaluating diet with a focus on less oily, fatty and fried foods. Regulating diabetes through diet, and increasing aerobic exercise (walking first, incline-based walking next, swimming or any low-stress cardiovascular activity. Light resistance training).
Annual carotid tests are a must. Prolonged rehab and aerobic work boosts chances of stroke-free survival to over 90% at 5 years.
Questions to Ask Your Doctor
Unlike a simple physician visit, CAS is a procedure that can be quite anxiety-inducing and emotionally draining. It can naturally evoke some questions. Here are some to ask your doctors, if CAS has been indicated:
About your specific diagnosis:
- How severe is my artery narrowing (percentage stenosis), and what test confirmed it?
- Am I symptomatic (TIA/stroke) or asymptomatic, and how urgent is this?
Procedure details:
- Why CAS over surgery (endarterectomy) for me — my anatomy, health risks, or prior radiation?
- What stent type and protection device (filter/flow reversal) will you use?
- How long will the procedure take, and can it be via wrist (radial) access?
Risks and alternatives:
- What's my personal stroke risk during/after CAS vs. doing nothing or surgery?
- How is this assessed? How long must I take dual antiplatelets, and what if I have bleeding risks?
Recovery and follow-up:
- When can I drive, work, or exercise? Any rehab plan?
- What follow-up scans/tests, and signs to watch (headache, weakness)?
Long-term:
- Expected stent durability and lifestyle changes needed?
- How do I manage any potential signs of trouble, if I’m living alone?
- Are there any activities that I absolutely have to avoid, for life?