

Aortic Valve Replacement Surgery
 Home
Home- Aortic Valve Replacement Surgery

Medically Reviewed By Dr. Vishal N. Pingle, Cardiothoracic & Heart Transplant Surgeon. Updated on March 24, 2026
Aortic heart valve replacement (AVR) surgery treats severe aortic valve diseases, mainly benefiting the heart function and thereby, quality of life. The surgery addresses conditions like aortic stenosis and aortic regurgitation through traditional open-heart surgery or minimally invasive options like TAVI/TAVR.
The aortic valve is the heart’s gateway to the body. It can narrow through aortic stenosis or leak through regurgitation. These cause fatigue, breathlessness, chest pain or even fainting — typical cardiac symptoms. While traditional open-heart surgery replaces the valve via a chest incision, TAVR delivers a new valve through a leg artery catheter, ideal for higher risk patients.
Conditions Treated by Aortic Heart Valve Replacement (AVR) Surgery
Aortic valve replacement (AVR) surgery targets two major conditions affecting the aortic valve: aortic stenosis and aortic regurgitation.
Aortic stenosis:
Aortic stenosis results from the narrowing of the aortic valve, like a clogged pipe, restricting blood flow to the body. Calcium buildup stiffens the valve leaflets (whose optimum functioning depends on elasticity), forcing the heart to work harder to pump blood through the valve. The resulting symptoms are chest pain (angina), breathlessness during physical activity, persistent fatigue, lightheadedness and seemingly sudden fainting spells (syncope). Left untreated, the heart muscle gradually weakens, risking heart failure.
Aortic regurgitation (insufficiency):
Aortic regurgitation happens when the valve — which regulates direction of flow doesn’t close tightly — letting blood leak backward into the heart. This causes the heart to enlarge as it overcompensates, resulting in symptoms like palpitations, breathlessness (especially when lying down), extreme fatigue and swelling in the legs and abdomen. Both these conditions impair daily life, robbing one of the ability to perform simple tasks like walking or climbing stairs. Early signs mimic symptoms of ‘aging’ (sometimes an overtly generalized explanation for things), however, echocardiograms reveal the extent of the issue. AVR replaces the faulty valve with a new one (mechanical or tissue), restoring efficient blood flow, easing symptoms and preventing progression. Many patients regain strength and vitality in a matter of weeks.
Indications to Perform Aortic Heart Valve Replacement (AVR) Surgery
Aortic valve replacement surgery is advised when the aortic valve issue becomes serious enough to threaten overall heart health. Here’s what that means for patients:
First, doctors have to confirm severe aortic stenosis (the most common cause), through an echocardiogram and other tests. If there are symptoms like severe chest pain, syncope (passing out), or any signs of heart failure (shortness of breath, swelling in the lower extremities and severe fatigue), surgery is strongly advised. These symptoms signal that the heart is not pumping blood efficiently, and waiting can lead to irreversible damage.
Aortic regurgitation is also detected through the echocardiogram. Transthoracic echo used ultrasound waves on the chest to evaluate the leaflets, estimate the severity of the leak by colour Doppler studies (backward jet), and examine the left ventricle size and function. It quantifies leakage with metrics like regurgitant volume (>60 mL = severe) or effective regurgitant orifice (>0.4cm² = severe). If needed, transesophageal echo (TEE) gives clearer images by inserting a probe down your throat, especially for endocarditis or aortic root issues.
Even without symptoms (asymptomatic cases — common in diabetics, as diabetes tends to mute classic symptoms due to a systematic destruction of the autonomic nervous system), AVR may be required if tests show a weakening heart.
Key red flags include:
- Left ventricular dysfunction: Your heart’s main pumping chamber isn’t squeezing well enough, with an ‘ejection’ fraction below 50% (normal range is 50 to 70%) .
- Very narrow valve: An aortic valve area of less than 0.6 cm², which is a critical bottleneck.
- High pressure gradients: More than 60 mmHG across the valve, meaning the heart is working overtime.
Recommendation by experts, such as the American Heart Association, recommend TAVI/TAVR procedure (Transcatheter Aortic Valve Replacement) for high-risk patients who are above 75 years of age, with lung problems, frail, and with any previous history of surgeries. Open-heart surgery comes with other risks, which could be counter-productive.
TAVR involves the use of a catheter through the leg artery (thereby avoiding a big incision) and speeding recovery. Cardiologists typically assess age, fitness levels and risk factors to decide which option is the best to regain energy and avoid emergencies.
Step-by-step guide to Aortic Heart Valve Replacement (AVR) Surgery
AVR has two forms: the traditional open-heart surgery (SAVR) or the transcatheter approach (TAVR). As mentioned above, doctors decide on an approach based on the patient's risk profile. Age, severity of the condition, and other comorbidities are factored in, while weighing benefits and outcomes. Here’s what one can expect from either approach:
Preparation: In general, overnight fasting is required. IV lines are inserted for fluid and medication administration. Both procedures are performed under general anesthesia, which renders a patient unconscious. A breathing tube will assist in respiration.
For SAVR (open surgery, 2-4 hours): The surgeon makes an incision in the chest, divides the breastbone (sternotomy), and opens the heart sac. The patient is usually attached to a heart-lung machine, which will oxygenate blood while the heart is safely stopped. The aorta is opened, faulty valve removed, debris cleaned and then, a new valve is sewed back in. The aorta is then closed, and the heart is turned back on (sometimes with a shock); the patient is finally weaned off the machine and the chest is closed with wires or stitches.
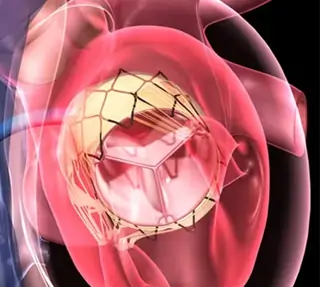
For TAVR (1-2 hours): No chest incision — a small groin incision (femoral) is used to guide a catheter with X-ray and echocardiogram. Doctors balloon dilate the old valve, place and expand a new one inside the old one, check for fit, and then, withdraw the catheter. For more detailed article on TAVI/TAVR procedure click here.
Advanced Techniques in Aortic Heart Valve Replacement (AVR) Surgery
Minimally invasive approaches now allow for surgery with small thoracotomy incisions (6-7 cms) for direct access, and significantly lower infection risks.
Rapid-deployment valves: These ‘snap-in’ tissue valves use a balloon to expand, reducing surgery time and bleeding.
Ross Procedure: For younger patients, they swap the aortic valve with the pulmonary valve (plus a donor pulmonary), so there’s no need for blood thinners for life.
Hybrids: Like HCR (Hybrid Coronary Revascularization), which is a combination of minimally invasive CABG Surgery and angioplasty, surgical and catheter approaches are used for aortic conditions too. Surgical teams take these calls based on the coronary anatomy, and overall risk profile.
Benefits of AVR Surgery
Aortic Valve Replacement can transform life quality by addressing the root cause of multiple symptoms and protecting long-term heart health. AVR replaces a faulty valve with either a mechanical one (made of metal, lifelong durability but requires blood thinners) or tissue (from pigs or cows, no blood thinners needed but the durability is 10-15 years). Either of these restore smooth blood flow, halt the progression of heart failure, and significantly improve survival outcomes — many patients live 10-20+ years of active life after the surgery.
Some of the benefits include increased enthusiasm for walking and other physical work like gardening, or even spending time with family. Hemodynamics are greatly enhanced, making exercise, light sport and travel possible without constant dizziness or fatigue.
Of the different approaches, TAVR shines for quick wins: Just 1-3 days in the hospital as compared to 5-7 days for SAVR, with less pain and fatigue. Driving and work can resume in weeks, not months. SAVR patients often take 6-12 weeks to fully recover with rehab.
Risks & Complications of Aortic Heart Valve Replacement (AVR) Surgery
There are risks associated with every surgery and aortic valve replacement (AVR) is no different. But modern technology is lowering these risks. Put in context, the risks of living with a dysfunctional valve are significantly higher.
Common risks (1-5%): Bleeding requiring a transfusion, irregular heartbeats (arrhythmias such as AFib, which may be temporary), infection at the incision sites, or stroke due to blood clots or air bubbles. Blood clots can form, therefore, patients are given blood thinners short-term.
Serious but rarer problems (<2%): Leak or malfunction of the valve, heart block requiring a pacemaker, strain on the kidneys from bypass (TAVR eliminates this), or fluid accumulation in the lungs. The long-term problem with mechanical valves (as opposed to tissue valves) is clot formation (hence, anticoagulants). Tissue valves can wear out, requiring redo surgery.
TAVR specifics: Damage to an artery or valve misplacement (corrected during the procedure). Open surgery also comes with a risk of infection, and pain from healing the sternum or inflammation from bypass.
Over 90% of patients go through AVR with no problems at all. Comprehensive ICU monitoring, antibiotics, and rehab spot/prevent problems early. Heart teams use risk scoring tools (such as STS risk calculator or EUROScore) to assess the merits against the disadvantages, and make decisions.
Recovery & Rehab
As mentioned earlier in the article, the after-effects of AVR are dramatic. Most patients feel worlds better within weeks. Here’s what that journey looks like:
Hospital stay: TAVR patients return home in 1-3 days, while SAVR patients return home in 5-7 days. ICU monitoring with a focus on heart rate, blood pressure and breathing is standard protocol.
Early days (Week 1): The patient will have chest tubes, IVs and pain meds. Deep breathing and coughing are practiced on an hourly basis to avoid any lung problems. By day 2, short walks with assistance are recommended — crucial to prevent clotting.
Weeks 2-6 (Home recovery): Until doctors give a go-ahead, lifting anything over 5-10 lbs or driving is not recommended. This period is about 4-6 weeks for SAVR patients. Walking time is gradually increased — starting at 5-10 minutes a day, and slowly progressing to 30 minutes. Heart-healthy eating (low salt, veggies and reduced oil intake) is obviously recommended, and weight is closely tracked to look for fluid retention.
Weeks 8-12 (Cardiac rehab): This included supervised exercises, education on meds (like blood thinners) and stress management (very important for a recovering heart). At this stage, 150 mins of moderate aerobic activity weekly is the goal.
Follow-ups check valve function via echo. Most resume normal life by 6-12 weeks — energy returns, stairs get easier, work commutes are possible. However, it is crucial to listen to one’s body and look for swelling, fatigue, sudden fevers or palpitations.
India-specific stats:
India has a massive need for aortic valve replacement (AVR) that stands at 250,00 to 300,000 patients with severe aortic stenosis that can benefit from TAVR alone. This is more than the number of cases in Europe and North America combined. This stems from our 70 million elderly population and the increasing incidence of degenerative valve disease, which is now the leading cause of isolated aortic stenosis (4.8% of valve disease), surpassing rheumatic heart disease.
Due to the lack of consolidated heart valvular disease registries, regional patterns are hard to track and any data available often reflects the reports from big cities and super-speciality centres. Any estimates are merely extrapolations from hospital studies and demographics — no granular state-wise breakdowns exist yet.
Questions to ask your doctor:
- Is AVR urgent, or can we monitor for longer?
- What happens if I delay?
- Procedure options — SAVR, TAVR or minimally invasive?
- Which one is best for me and why?
- Will the replacement be a mechanical valve or tissue valve? What are the benefits of either? And, will I require blood thinners?
- What are my personal risks? How are these assessed?
- If I choose to avoid the surgery, what are my options?
- What activities should I avoid after surgery?
- What specific modifications in diet should I make? Before and after?