

Varicose Veins
 Home
Home- Varicose Veins

Medically Reviewed By Dr. Karan Anandpara Updated on February 23, 2026
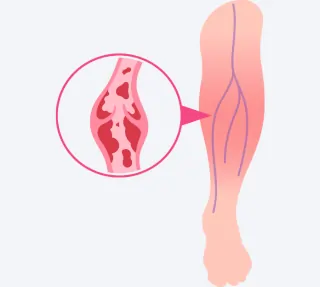
Varicose Veins are essentially swollen, twisted veins (almost worm-like in their appearance), visible under the skin. They’re caused due to weakened vein walls and faulty valves; these allow blood to pool (collect) and in turn cause bulging (which gives the veins the twisted appearance) and discomfort.
In most cases, varicose veins are visible in the legs due to the gravity’s impact on blood flow. They can present elsewhere in the body in rare and very specific cases. The rectum, arms and hands, oesophagus and pelvis/genital area are among the less common areas.
Causes of Varicose Veins
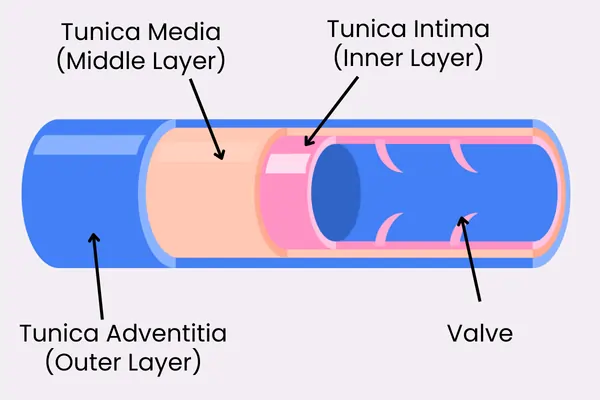
To understand why varicose veins are caused, we need to understand the role of valves in blood vessels. Vein valves are one way flaps (think of them like sluice gates of a dam) inside veins that facilitate blood flow towards the heart, against gravity. They prevent backflow, especially in the legs.
Blood pressure opens the cusps towards the heart, during a muscular contraction. Reverse pressure (stasis) closes them, sealing the edges to block any reflux. Each valve consists of two thin, flexible cusps or leaflets. They’re made of collagen, covered by endothelium and project from the vein wall. Usually, they form in pairs, more numerous in distal leg veins like the Greater Saphenous Vein (10-20 in these) and fewer proximally.
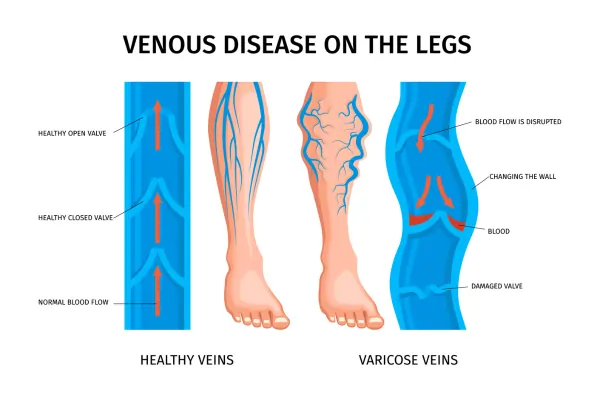
When the leaflets get weakened, their ability to close is compromised. This incompetence causes reflux, venous hypertension and the dilation of superficial tributaries. While there are multiple reasons for this weakness, age, trauma and clots are the most common factors influencing this.
Once backflow occurs, it collects in bulges or pools called varicosities. These, in turn, cause the swelling and twisted appearance.
Here’s a breakdown of the factors causing valve weakness, reflux and hence, varicose veins.
Primary factors: Valve can fail without prior injury. Vein walls tend to dilate first due to genetic weakness, age or hormones. This pulls the valve leaflets apart, so they can’t close properly.
Secondary factors: Deep Vein Thrombosis (DVT) has an impact on valves. It scars them; the resulting inflammation activates enzymes that degrade leaflets.
Congenital factors: Very rarely, there are malformations from birth. This accounts for 1-3% of cases.
While not causative, there are other contributing factors: Prolonged standing or sitting, obesity, pregnancy and family history all increase venous pressure, thereby hastening wear of leaflets. The reduced blood flow ‘switches on’ certain genes creating a self-perpetuating cycle of reflux and hypertension.
How do valve-maintaining genes work?
Reduced blood flow disrupts shear stress signals that typically activate genes necessary for venous valve maintenance (survival, essentially). The reduced blood flow slowly ‘switches’ off these genes, causing leaflets to start failing. This in turn causes a faulty remodeling of the valves and veins.
Blood flow generates laminar shear stress on the valve endothelial cells. Eventually, the activated pathways, along with gap junction genes promote leaflet elongation, proliferation of valve-forming cells and organization. Without blood flow, these processes are halted, resulting in a cycle that slowly ‘shuts off’ or ‘silences’ crucial genes.
Symptoms of Varicose Veins
The early stages of varicose veins don’t show visible changes, but involve discomfort. Later stages show skin damage and ulcers. The progress is measured in accordance with the CEAP classification (C0-C6).
Early stages (C0-C2)
C0: Shows no visible signs, with symptoms mimicking other conditions like pitting edema. Achy and tired legs after standing, for long. This stage is often ignored, due to the very generalized nature of symptoms. It’s mainly subtle fatigue, indicating reduced blood flow.
C1 (spider/reticular veins): Mild itching or burning. Small vessels appear, without bulging.
C2: The first prominent stage of varicose veins. Twisted, bulging, purple-blue cords on legs. Aching, throbbing, cramps (at night), and restless legs which worsen towards the end of day.
Intermediate stages (C3-C4):
C3 (Edema): There’s heaviness around the ankles, pitting on pressure and heaviness that persists despite elevation.
C4 (Skin changes):Dry/thin skin, itching, reddish-brown discolouration and eczema like dermatitis. Legs tend to feel warm.
Late stages (C5-C6):
C5: Scarring at the ankle area, from prior sores. Skin tends to harden (lipodermatosclerosis).
C6 (Active ulcer): Painful open-sores near the medial ankle, slow healing with yellow slough and a high-risk of infection.
Treatment for Varicose Veins

Treatment choice is informed by the CEAP scale and obviously, patient factors (E.g., valve failure, risks, etc). For the most part, treatment is elective. In the earlier stages, symptom relief is often the focus. In the later stages, minimally invasive procedures may be considered, to address the underlying reflux.
Early-stage/conservative options:
These only manage symptoms, without curing reflux. Compression stockings (20-30mmHG) are the most common short-term approach; they improve blood flow and reduce swelling/aching. Leg elevation on a wedge pillow, exercise (walking) and avoiding prolonged standing also offer some relief.
Minimally Invasive procedures:
These are considered as a first-line approach for C2+ cases. They target the saphenous reflux via catheter.
Endovenous thermal ablation: EVLT Procedure (laser) or RFA (Radio Frequency Ablation) heats/closes faulty veins with a 95% success rate.
Sclerotherapy: Foam injection which scars branch veins; this is ideal for residuals post ablation.
VenaSeal (glue): Cyanoacrylite seals without heat.
There are more advanced surgical options (for E.g, ambulatory phlebectomy) that are used for large tortuous (curved) veins; however, these are rarely resorted to due to the high success rates of endovenous treatments.
Risk Factors for Varicose Veins
Risk factors can be broadly divided into modifiable and non-modifiable.
Non-modifiable:
Age: After the age of 55, elasticity tends to fade, leading to an increased risk.
Gender: Females have a 2-3x higher risk, due to hormonal changes (pregnancy, estrogen, etc.)
Height: Leg vein pressure is increased in taller people.
Genetics: Family history is considered a factor by some. While there is evidence to suggest that varicose vein heritability exists, its specific impact on venous valve function still requires some detailing.
Modifiable:
Pregnancy: While not exactly ‘modifiable’, pregnancy combined with a genetic predisposition does pose a significantly increased risk. During pregnancy, a combination of hormonal, mechanical and hemodynamic effects exert a strain on valves and vein walls. Increased blood volume stretches vessels and tends to cause pooling. A growing womb presses on the pelvic veins, thereby elevating venous pressure. Furthermore, hormonal relaxation due to increased progesterone/estrogen levels relaxes smooth muscle in vein walls, worsening reflux.
Obesity/High BMI: Compresses veins, and thereby worsens reflux.
Prior DVT: Scarring causes secondary failure.
Occupational stress: Prolonged standing/sitting due to the nature of work reduces shear flow. This, in turn, can result in compromised valves and vein walls.
Smoking and hypertension: Amplifies inflammation and venous pressure.
Varicose Veins — Prevalence Across India
| Region/Area | Prevalence/Notes | Susceptibility Factors |
|---|---|---|
| Northern India (Uttar Pradesh villages) | 46.7% females, 27.8% males (C1+); 49.3% venous symptoms in women. | Heavily physical occupations, age >40. |
| Karnataka (Dakshina Kannada/Sullia) | 74% males; 40% farmers; common in 41-50 age group. | Heavily physical occupations, left leg dominance (70%). |
| Healthcare workers (nationwide, e.g., nurses) | 24.1-48.8%; up to 86% female in some surveys. | Prolonged standing, urban hospitals. |
| Mangalore (South India) | Male predominance (84%); occupation-driven. | Similar to Karnataka, with a specific tilt towards coastal occupations. |
These findings are based on studies conducted across different centers in the Southern and Northern parts of India. While not conclusive, they do offer some insight into basic patterns. North East India and the mountain regions remain understudied, to draw any conclusive patterns.
Prevention of Varicose Veins
Largely, prevention strategies focus on countering modifiable risks such as prolonged stasis, obesity and poor circulation which increases valve stress.
From a lifestyle perspective, the first step is maintaining a healthy weight. Even losing 3-4 kilos eases the strain on veins. To function well, valves need shear stress, which is best offered by aerobic and anaerobic exercises. Walking, running, cycling, resistance training, and targeted work on the calves can help. The other key aspect is to avoid standing or sitting for prolonged time periods. Ideally, a break every 30 minutes would help. Flexing the ankles while sitting and keeping the legs elevated while resting improves blood flow.
Evidence indicates that calf-strengthening can reduce early risks by as much as 50%. Here are some sample exercises that can be considered:
Calf-raises: This strengthens the pump for upward blood flow. Around 3 sets of 20-30 reps should suffice.
Brisk walking: The focus should be pace, over distance. Even 30 minutes at a sustained or gradually increasing pace is very helpful in reducing edema.
Swimming: If possible, nothing like it! The hydrostatic pressure aids circulation, like natural compression.
Leg lifts: A core-training basic. Gravity drains pooling. About 12-20 repetitions with a 5 second hold, should do.
Ankle flexes: An engaged and pointed rotation of the toes. About 20/side. This is particularly useful for those who spend a lot of time on a desk. Prevents stasis.
Yoga/Pilates: While a bit lower on specificity, these definitely benefit overall circulation. Core-focused poses, in particular, aid this.
Extremely heavy resistance training (1-3 rep maxes), and high-impact movements (the use of power and impact-on-contact) need to be practiced very carefully. Preferably, phased into.
In addition to these changes, supportive measures are needed. From a dietary perspective, high-fiber and low-salt intake helps. Compression stockings (15-30mmHg) prevents pooling; these can be worn especially during activities that involve standing or sitting for extended periods. While marginal in impact, clothing choice can also help. It is strongly recommended to avoid tight waistbands and high-heels.
Complications if Not Treated
While rarely fatal, varicose veins can impair mobility and quality of life. In some cases, ruptured veins can lead to bleeding. Ongoing reflux, venous hypertension and clotting can progress into more serious complications.
In the C1-C3 stages, if left untreated varicose veins can cause pain, a worsening swelling, and eventually hardened skin (lipodermatosclerosis) that’s itchy, fragile and prone to tears.
In the later stages, C4-C6, there can be open sores at the ankle which are slow healing and infection prone.
Sometimes, superficial clots can extend to deeper veins causing DVT (Deep Vein Thrombosis), which in turn poses serious risks like pulmonary embolism. In extremely rare cases, ruptures can cause massive hemorrhage.
Questions to ask your doctor:
- What causes my varicose veins?
- What stage is my condition on the CEAP scale?
- How do I know this isn’t deep vein thrombosis (DVT)? What are the key differences?
- What tests do I need?
- What sort of treatment suits me, and why?
- What are the recovery rates for patients of my profile?
- How will this affect my pregnancy plans?